What Is Synapse Health?
Synapse Health is not a traditional DME provider. They do not warehouse equipment or employ trained delivery staff. Instead, they broker services by sub contracting with outside DME companies to fulfill orders.
What Happens Next? ONeal Medical CPAP-Plus will:
Coordinate pickup of our rental equipment August and September of 2025.
Facilitate delivery from the new subcontracted DME provider assigned by Synapse (TBA).
Continue to serve patients with the highest standard of care until these transitions are complete.
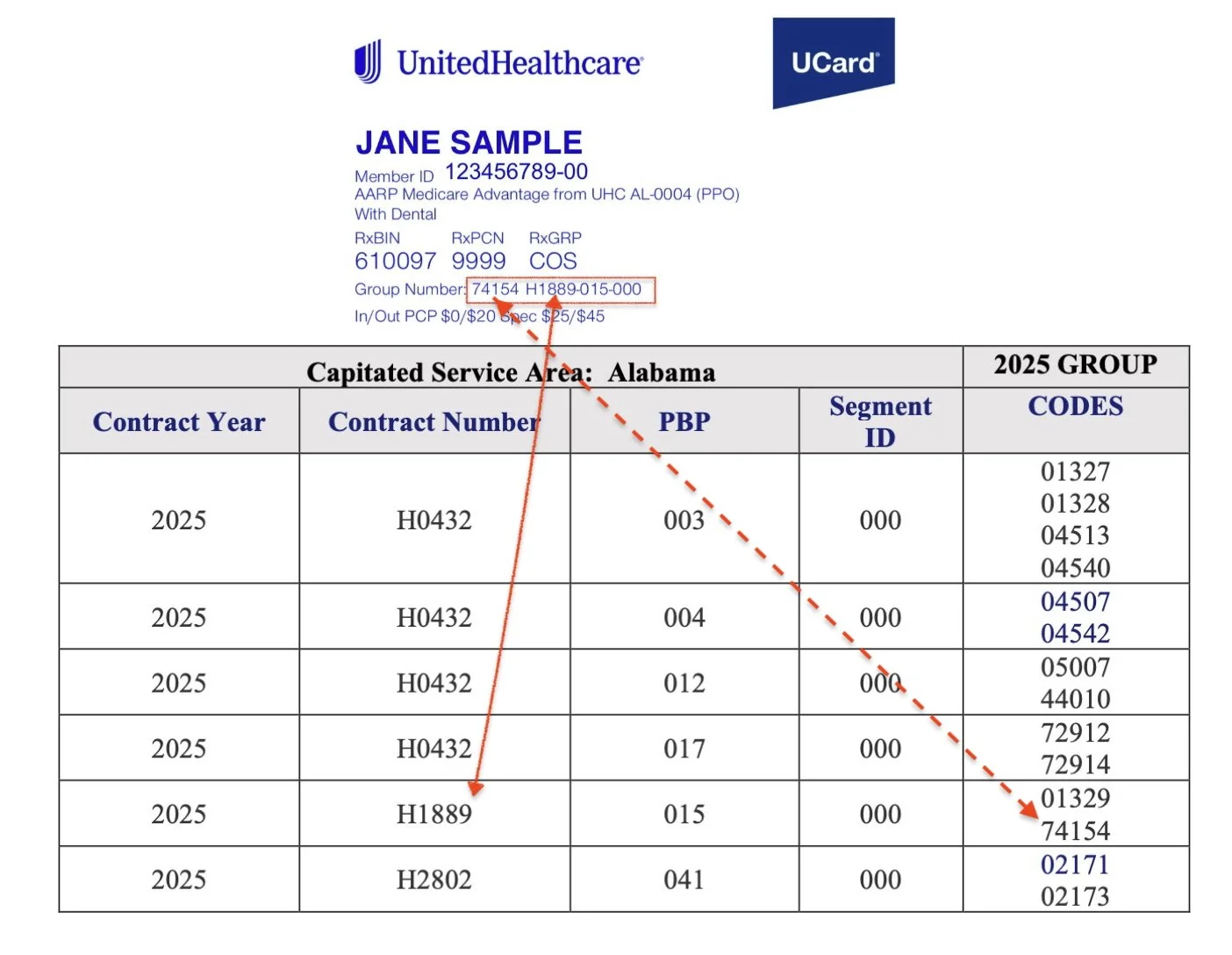
To find out what plans are affected: Check the United Healthcare UCard and look for:
Group Code/Number
Contract Number
If the patient’s UCard has either the Contract or Group number below, the patient must use Synapse Health for their DME by calling:
1.888.33.MYDME
(1.888.336.9363)